July 14, 2026
Status: Almost Recruiting
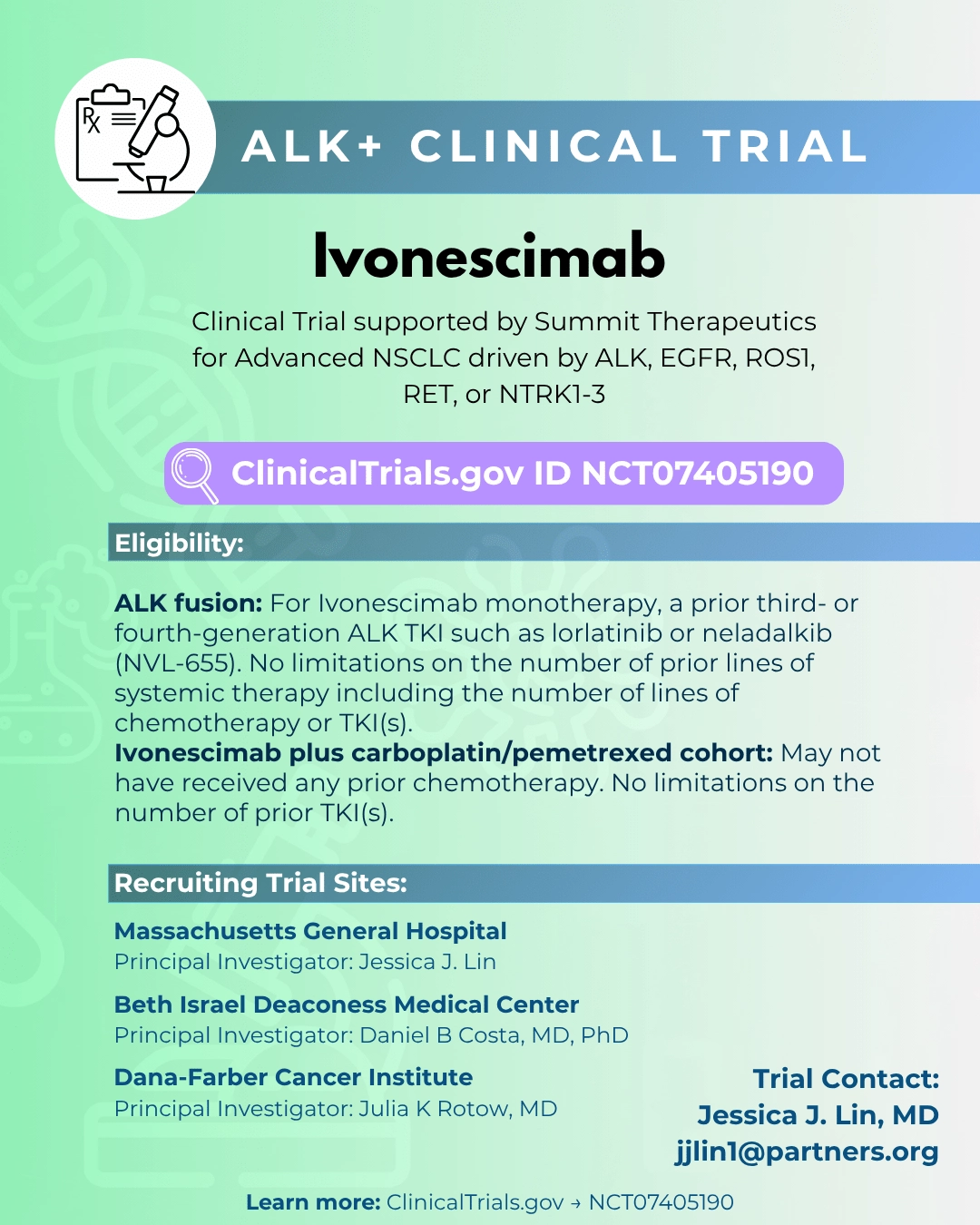
Phase: Phase 2 Study of Ivonescimab (AK112) Alone and With Carboplatin/Pemetrexed For Advanced NSCLC With Actionable Genomic Alterations Including ALK+ NSCLC
Drug: Ivonescimab (AK112) with Caroboplatin/ Pemetrexed
Purpose of this Clinical Trial
This Phase II clinical trial evaluates the efficacy and safety of ivonescimab (AK112) in patients with advanced non-small cell lung cancer whose tumors harbor actionable oncogenic driver alterations, including ALK rearrangements. The study is designed as a biomarker-driven basket trial that enrolls multiple molecular subsets, including ALK, ROS1, RET, NTRK, and selected populations with EGFR-mutant lung cancer. The ALK cohort is one component of a broader precision oncology strategy rather than a dedicated ALK-only study. Ivonescimab is a bispecific antibody that simultaneously targets PD-1 and VEGF, combining immune checkpoint inhibition (removing the brakes on the immune system) with anti-angiogenic modulation (inhibiting tumor blood vessel growth) in a single therapeutic agent. Treatment is administered intravenously on a repeating scheduled cycle, with some cohorts receiving ivonescimab alone and others receiving it in combination with platinum-based chemotherapy depending on prior therapies and study arm assignment.
Who This Trial is For (ALK Cohort Focus)
The ALK cohort is intended for patients with histologically confirmed advanced or metastatic ALK-positive non-small cell lung cancer who have previously been treated with standard ALK tyrosine kinase inhibitors. In most cases, this includes prior exposure to second and third-generation ALK inhibitors such as alectinib, brigatinib, and lorlatinib. Many patients considered for this cohort are in the post-lorlatinib or post-next-generation ALK inhibitor setting where standard targeted therapy options have been exhausted or are no longer providing durable disease control. Patients must have measurable disease, adequate organ function, and sufficient performance status to receive systemic therapy. This cohort is generally designed for patients for whom no satisfactory targeted therapy options remain and where chemotherapy has historically been the default standard of care.
Scientific Rationale
Immunotherapy has historically shown limited efficacy for ALK-positive non-small cell lung cancer. This is largely attributed to the biologic characteristics of ALK-driven tumors, which typically have low tumor mutational burden, limited neoantigen formation, and a tumor microenvironment that is immunologically “cold.” As a result, PD-1 or PD-L1 inhibitors alone have demonstrated low response rates in this disease setting, particularly after exposure to ALK tyrosine kinase inhibitors. Ivonescimab is designed to address this limitation through simultaneous inhibition of PD-1 and VEGF. The VEGF pathway plays an important role in tumor angiogenesis and also contributes to immune exclusion by creating abnormal tumor vasculature and suppressing T-cell penetration into the tumor microenvironment. By blocking VEGF in addition to PD-1, ivonescimab is intended to normalize tumor blood vessels, enhance immune cell infiltration, and reduce the immunosuppressive effects of VEGF signaling. This dual mechanism is hypothesized to convert an immunologically inactive tumor environment into one that is more responsive to checkpoint blockade. In ALK-positive disease specifically, VEGF-mediated immune exclusion may represent a key barrier to immunotherapy response even after oncogenic signaling is suppressed with ALK inhibitors. The rationale for this study is therefore not that PD-1 blockade alone will suddenly become effective in ALK tumors, but rather that VEGF inhibition may unlock immune access and allow PD-1 inhibition to exert meaningful antitumor activity.
Trial Design Overview
This study is structured as a multi-cohort Phase II basket trial that evaluates ivonescimab across several oncogene-defined NSCLC populations. In addition to ALK-positive NSCLC, the trial includes cohorts for ROS1, RET, and NTRK rearrangements as well as selected EGFR-mutant populations. The design reflects a broader effort to evaluate whether dual PD-1 and VEGF inhibition has activity across multiple oncogene-driven tumor types that have historically been resistant to immunotherapy alone. Treatment is administered as intravenous ivonescimab on a repeated cyclic schedule. Some cohorts include combination therapy with platinum and pemetrexed chemotherapy, while others evaluate ivonescimab monotherapy depending on prior treatment exposure and cohort assignment. Tumor assessments are performed using RECIST 1.1 criteria with scheduled imaging intervals.
Endpoints
The primary endpoint of the study is objective response rate as defined by RECIST 1.1 within each molecular cohort, including the ALK population. Secondary endpoints include progression-free survival, duration of response, disease control rate, and safety and tolerability. The study also evaluates intracranial activity in patients with central nervous system metastases, which is particularly relevant in ALK-positive NSCLC given the high incidence of brain involvement in this disease.
Inclusion and Exclusion Criteria
Patients eligible for the ALK cohort must be adults with histologically confirmed advanced or metastatic non-small cell lung cancer and a documented ALK gene rearrangement. They must have received prior systemic therapy, including at least one ALK tyrosine kinase inhibitor. Receipt of multiple prior lines of ALK-targeted therapy is allowed. Patients must have measurable disease, adequate bone marrow, hepatic, and renal function, and an Eastern Cooperative Oncology Group performance status that allows for systemic therapy. Patients are excluded if they have uncontrolled autoimmune disease requiring immunosuppression, prior severe immune-related toxicity from checkpoint inhibitors, uncontrolled central nervous system disease that does not meet protocol criteria for stability, or concurrent participation in another interventional clinical trial. Patients with significant uncontrolled comorbid illness that would interfere with protocol therapy are also excluded.
Scientific Positioning in the ALK Treatment Landscape
This trial occupies a unique position in the evolving treatment landscape for ALK-positive non-small cell lung cancer. Unlike ALK tyrosine kinase inhibitors, which directly target the oncogenic driver, ivonescimab represents an immune and microenvironment-directed strategy. It is therefore not intended to replace ALK inhibitors but rather to serve as a potential option after exhaustion of targeted therapy. In practical terms, the study is most relevant to patients who have progressed after second-generation and third-generation ALK inhibitors, including lorlatinib, and who may have limited remaining targeted options. In this setting, chemotherapy has historically been the standard treatment, but outcomes are generally modest. This trial explores whether dual PD-1 and VEGF inhibition can provide an alternative systemic approach in this post-TKI setting. As newer generations of ALK therapies, including next-generation inhibitors and ALK degraders, continue to emerge, the role of immunotherapy-based strategies remains uncertain. However, this study tests a biologically rational hypothesis that modifying the tumor microenvironment may allow immune therapy to play a meaningful role even in oncogene-driven disease.
Strengths and Limitations
The primary strength of this study lies in its novel mechanism of action, combining immune checkpoint blockade with VEGF inhibition in a single agent. This dual approach is designed to address one of the central barriers in ALK-positive NSCLC, which is immune exclusion driven by tumor vascular and microenvironmental factors. The study also benefits from a biomarker-driven design and includes evaluation of central nervous system (CNS) disease. Limitations include the early phase nature of ALK-specific data, as well as the inherent complexity of basket trial designs. In addition, while the biological rationale is strong, immunotherapy in ALK-positive disease has historically been unsuccessful, and it remains uncertain whether VEGF co-inhibition will be sufficient to overcome this resistance in a clinically meaningful way. The optimal sequencing of this approach relative to emerging fourth-generation ALK inhibitors and ALK degraders also remains undefined.
Summary
Clinical trial NCT07405190 represents a next-generation immunotherapy strategy for oncogene-driven non-small cell lung cancer, including ALK-positive disease. By combining PD-1 blockade with VEGF inhibition, ivonescimab is designed to address the immune exclusion characteristics that have historically limited the effectiveness of checkpoint inhibitors in this population. For ALK-positive patients, this study is most relevant in the post-ALK inhibitor setting where standard targeted therapies have been exhausted and chemotherapy remains the primary option. While still investigational, the trial explores whether modifying the tumor microenvironment can create a therapeutic window for immunotherapy in a disease that has traditionally been considered non-immunogenic. As the ALK treatment landscape continues to evolve with next-generation TKIs and degraders, this study will help clarify whether immune–vascular modulation has a meaningful role in extending treatment options beyond targeted therapy.
Initial Trial Locations
Massachusetts Locations
Massachusetts General Hospital
Contact: 617-724-4000 jjlin1@partners.org
Co-Principal Investigator:
Jessica J Lin, MD 617-724-4000 swaliany@mgh.harvard.edu
Co-Principal Investigator:
Sarah Waliany, MD, MS
Beth Israel Deaconess Medical Center
Contact: 617-667-9236 dbcosta@bidmc.harvard.edu
Principal Investigator:
Daniel B Costa, MD, PhD
Dana-Farber Cancer Institute
Contact: 617-632-6555 Julia_Rotow@DFCI.HARVARD.EDU
Principal Investigator:
Julia K Rotow, MD
View Full Trial Details on ClinicalTrials.gov
Clinical trial details may change. Please refer to ClinicalTrials.gov for the most up-to-date information.
Jeffrey M. Sturm BS, MA, MBA
ALK Positive, Inc. www.alkpositive.org
Member, Medical Committees
Member Board of Directors
Clinical Trials Connect Editor and Moderator
Eleven-year ALK NSCLC survivor